The Project
Our work program
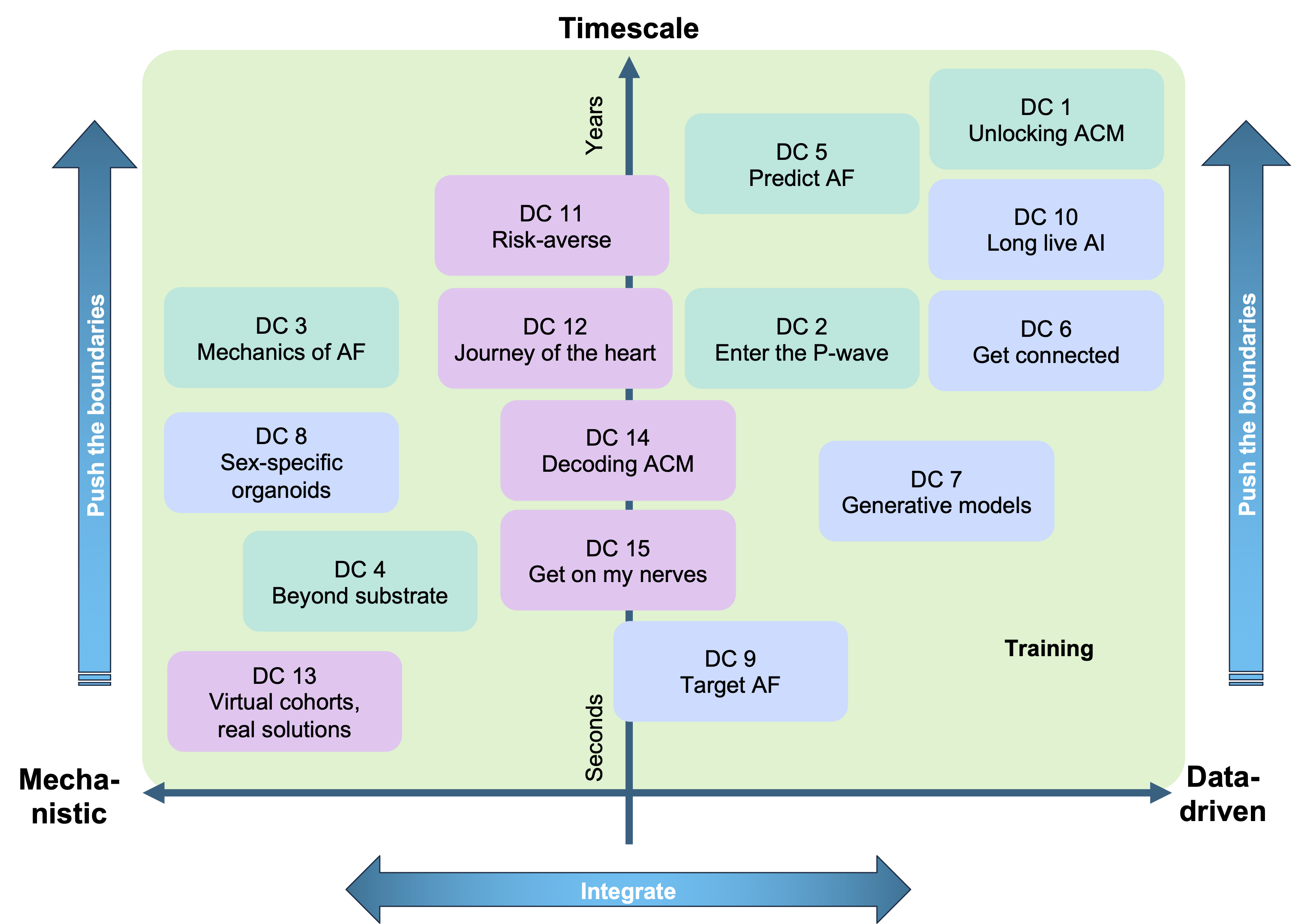
Three interconnected work packages, each addressing a critical stage of AF management: before diagnosis, immediately after the initial diagnosis, and progression/regression of the disease form the backbone of TrackAF’s research. The overall goal of TrackAF is to develop better tools, models and treatment strategies for AF and ACM across different time scales and patient populations, integrating the impact of non-modifiable AF risk factors age and sex, and their interaction, while also considering (partially) modifiable factors such as the lifestyle, diet, physical activity, exposome, socioeconomic status and epidemiological variation.
WP1: Before the Diagnosis focuses on early detection of AF, risk stratification and modification (i.e., prevention) by exploiting deep patient phenotyping and predictive biomarkers strongly linked to mechanistic models to identify patients at high risk of developing AF.
WP2: Immediately After the Initial Diagnosis is dedicated to improving diagnostic accuracy and treatment personalisation including lifestyle interventions and novel therapeutic strategies like PFA.
WP3: AF Progression and Regression addresses the long-term management of AF, focusing on strategies to track AF status, attenuate AF/ACM progression and promote AF/ACM regression.
| WP1 - Before Diagnosis | WP2 - At Diagnosis | WP3 - Progression and Regression |
|---|---|---|
| The variable occurrence of AF episodes and poor correlation between heart rhythm and symptoms make the early diagnosis of AF challenging, although there is increasing recognition that early diagnosis and treatment of AF is essential for improving outcomes and reducing costs. Accumulating evidence suggests that AF is a result of diseased atria (ACM) with pronounced sex differences and ageing as a major contributing factor. WP1 focuses on improving the (early) diagnosis and prevention of AF through risk prediction and management and a better understanding of the components of the ACM that modulate the risk of AF. WP1 integrates all major multidisciplinary methodological approaches, combining clinical research, experimental wet lab work, as well as ML and mechanistic modelling & simulation. We will employ high-quality data sets with biomarker information (wearable biosensors, ECG, imaging and clinical data) and AF characteristics that are available to various TrackAF partners to derive prediction models through statistical and AI approaches (DC1, 2). In addition, cellular experimental studies involving human atrial samples will be used to characterise the contribution of novel targets (e.g., mechanosensitive atrial remodelling) to ACM (DC3). Finally, mechanistic computer models will be used to obtain efficient surrogate atrial models that can be employed to rapidly evaluate AF inducibility (DC5) and characterise the determinants of ACM-related AF risk and the influence of the autonomic nervous system (DC4). | Once AF is detected, it is crucial to accurately assess and mechanistically understand the patient’s clinical condition before implementing any treatment strategy. While standard-of-care approaches, such as catheter ablation, can be effective in isolating AF triggers, detecting these triggers can be particularly challenging. There is no therapeutic consensus on how to treat patients, especially when triggers are located outside the pulmonary veins, . Additionally, factors like fibrosis and spatial heterogeneity within the ACM AF substrate play significant roles in the persistence of AF. These factors are highly patient-specific and can greatly influence the success of ablation treatments. WP2 aims to enhance the characterization of AF following diagnosis, to improve the prediction of treatment outcomes by accounting for inter-patient variability, including sex- and age-specific factors, and to refine existing treatment approaches through patient-specific modelling. To achieve these goals, WP2 will utilise multimodal clinical data available within the consortium to develop novel ML tools for stratifying AF patients (DC6) and predicting long-term treatment outcomes (DC10). Clinical data will be supplemented with new experimental data from induced pluripotent stem cells and cardiac organoids to further elucidate the role of sex and risk factors in AF (DC8). Using a latent representation of complex geometrical data, we will create generative AI models for simulation-ready cardiac anatomical models and virtual cohorts (DC7). The use of federated learning and latent data representation will also ensure anonymisation for a multi-centre approach. Additionally, we will explore new physics-informed methods for optimising ablation strategies in AF patients, where ECGI data will form the basis for defining an atrial digital twin (DC9). | AF and ACM are both progressive diseases and amenable to risk factor management , making it crucial to investigate their dynamic evolution over time, specifically in response to therapeutic/preventive interventions to better identify the most effective strategy for each patient. WP3 aims to create advanced decision-support models to understand the progression and regression of AF and ACM, with a particular focus on the impact of lifestyle factors (including physical activity, obesity, smoking, alcohol consumption and diet) to optimise treatment strategies, including personalised ablation and cardiac autonomic modulation as current strategies fail for persistent AF patients. This WP combines mechanistic and data-driven approaches across five specific projects (DC11-15). We will use patient-level models of AF that integrate risk factors such as hypertension, diabetes and sleep apnoea to reproduce the natural progression of the disease as a basis for in silico clinical trials (DC11). We will use clinical ECGI data obtained at different disease stages, at different times (before and after treatment) and from diverse populations to better understand dynamic response to therapy (DC12). Using virtual cohorts of bi-atrial digital twins, we will generate data for evaluating state-of-the-art mapping algorithms and help in the development of better mapping tools (DC13). In an established 3D mechanistic computer model of AF, we will introduce information from one of the world’s largest combined data sets of bulk mRNA and single nuclei sequencing to better understand the response to antiarrhythmic drugs (DC14). Finally, we will use computational tools to study how autonomic activity influences outcome in response to PFA and cryoablation (DC15). |
| WP4 - Training | WP5 - Communication, Dissemination and Exploitation | WP6 - Project Management |
|---|
Doctoral Projects
DC 1 - Unlocking ACM
Multimodal AF risk analysis and prediction of ACM in deep-phenotyped clinical cohorts
DC 8 - Sex-specific organoids
Influence of sex and risk factors in the development of AF by using cardiac organoids
DC 11 - Risk-averse
Assessing early comprehensive AF management using patient-level models of AF patterns and outcomes
DC 13 - Virtual cohorts, real solutions
Improving electro-anatomical mapping technology for better AF diagnosis and treatment